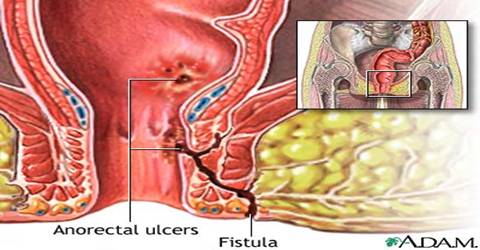
They arise after an infection in the
glands around the anal canal has caused an abscess which may have burst by
itself or required drainage by a surgeon.
Once the tunnel has formed they will
cause an intermittent discharge from the exit of the tunnel on the skin, this
may range from blood, to pus, to liquid to gas. The feeding source of the tunnel
is the entrance in the anal canal. If the exit of the tunnel closes over and the
entrance remains open then there will be a build up of contents in the tunnel
which cannot escape. The contents can then become infected and an abscess may
form which can then cause more damage to the surrounding tissues or lead to side
branches off the tunnel.
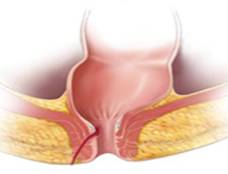
The tunnel will always pass through some
sphincter muscle around the anal canal, this maybe a small or large proportion
of muscle. The sphincter muscle is very important indeed as it keeps you
continent of gas and faeces. |
 |
Famous
patients with anal Fistulas
Hippocrates first described patients
with anal fistulas in approx 460 BC. The most famous sufferer was King Louis XIV (5 September 1638 ? 1 September 1715) - The Sun King.
His fistula was operated on by Charles Francois Felix on November 18th 1686. He required 4 further operations before being declared healed. Felix was
bestowed with an honorarium, an estate and a title (This is said to be the
highest paid fee for an operation in medical history). Charles Dickens was
plagued by a fistula and Shakespeare wrote about fistulas in ?All?s well that
ends well?
Classification of fistulas
Fistulas are named according to the Park's Classification
of Perianal Fistulas
| Transsphincteric fistulae are the result of
ischiorectal abscesses, with extension of the tract through the external
sphincter. Account for about 25% of all fistulae |
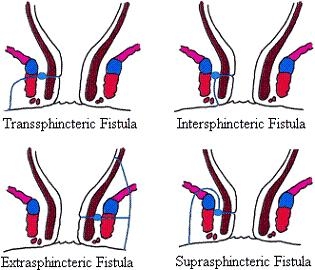 |
| Intersphincteric fistulae are confined to the
intersphincteric space and internal sphincter. They result from perianal
abscesses. Account for about 70% of all fistulae |
| Suprasphincteric fistulae are the result
of supralevator abscesses. They pass through the levator ani muscle, over the
top of the puborectalis muscle, and into the intersphincteric space. Account
for about 5% of all fistulae. |
| Extrasphincteric fistulae bypass the anal canal and
sphincter mechanism, passing through the ischiorectal fossa and levator ani
muscle, and open high in the rectum. Accounts for about only 1% of all fistulae |
TREATMENT OF ANAL FISTULAS
The best chance of cure is to ?Lay open?
the fistula, this involves cutting out the roof of the tunnel, scraping out all
the infected tissue, laying open any side branches and allowing the wound to
heal from inside out. However the tunnel always passes through muscle and
therefore some muscle will be cut. If one cuts muscle then the patient will have
their degree of continence control cut! The more muscle that is cut the more
control will be lost.
The muscle length ranges from 2 to 5 cm
long. Women have less muscle then men i.e. shorter anal canals. Also the muscle
between the vagina and anal canal is very thin and deficient in the deeper
aspects. This is further complicated by the fact that childbirth can weaken and
disrupt the muscles, nerves and supporting tissues. Approximately 25% of women
after childbirth will have a degree of incontinence usually to gas. It may be
that the amount of functioning muscle between the vagina and anal canal is only
1 cm (10mm) long.
Consider an anterior fistula (a fistula
whereby the exit of the tunnel is situated above an imaginary horizontal line
that divides the anus into 2 equal halves) that involves 3 mm of muscle. Should
this be laid open there is approximately a 30% chance of incontinence to gas and
liquid soiling and urgency to find a toilet. Patients often have to wear a pad
to absorb this discharge which may be the size of a 50p piece. |
Other techniques include
1. Seton insertion-Loose
2. Seton insertion-Tight
3. Advancement flaps
4. Fistula glue
5. Fistula Plug
6. LIFT procedure
7. Lay open and immediate repair of the
sphincter muscle. |
Unfortunately all techniques have a
failure or recurrence rate, this may range from 10-80%.
My Current techniques are as follows
1. Insertion of a loose seton to allow
drainage of all infection and control the fistula. This is also a recognised
treatment in itself as it prevents the exit of the tunnel closing over which may
cause a further abscess to form leading to further tissue/muscle destruction.
The seton therefore allows a continuous
discharge of contents which may require a small pad to be worn to prevent
soiling of underwear.
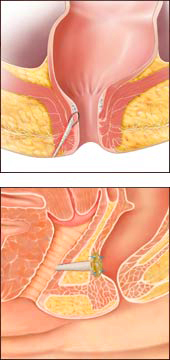
A seton is a stitch that is placed
through the tunnel, it is inserted under a general anaesthetic (The stitch is
like having a piercing of the bottom-lots of people have piercing of other body
parts!). The stitch is a fine piece of string that is soft or a fine elastic
band. In either case it is designed to to be soft and easy to sit on.
Patients are then reassessed to
determine how much muscle will be cut (laid open) and how much muscle will be
left behind that is functioning to keep continence. Further investigations are
sometimes requested (MRI, endoanal ultrasound scan). This allows informed
consent and discussion of surgical risks with the patient. I then proceed with
one of the following.
2. Lay open
3. Fistula Plug (currently private
patients only)
4. Lay open and immediate repair of
muscle. |
Advancement flaps.
I only perform this procedure rarely and in highly selected patients.
These may be associated with an up to
30% recurrence rate and 30% incontinence rate. |
| Fistula Glues.
These are now rarely performed due to the high (up to 80-100%) recurrence rates. |
| LIFT (Ligation of Intersphinteric
Fistula Track) is a new technique with no long
term results. It is an easy procedure which I can perform on selected patients |
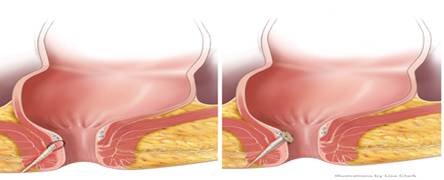
| Fistula Plugs.
(www.cookmedical.com/sur)
.These are only inserted after a loose seton
has been in place for at least 6 weeks and all infection has been eradicated.
Essentially a collagen plug is inserted into the fistula tunnel effectively
blocking the tunnel. The plug then provides a framework for the body tissues to
grow into and completely heal the fistula. This has a success rate of
approximately 50-70%. I am participating in a national randomised trial (FIAT
500) to evaluate the effectiveness of this new technique. The advantage of this
technique is no muscle is cut and therefore there is no loss of continence.
However failure rates are high and further abscesses may form which may cause
more tissue damage. |
Lay open and immediate repair of the
sphincter muscle. To date I have performed this
new technique on 7 patients (No recurrence and no incontinence after 2 year
follow up). This is a new technique that is performed on selected patients after
insertion of a loose seton and all infection has been eradicated.
Essentially the fistula anatomy is
dissected out, all the muscles are identified and mobilised. The fistula is laid
open and all side branches dealt with. The muscle is then repaired with an
overlapping technique. The lining of the rectum/anal canal is then advanced over
the repair closing the entrance to the tunnel. The skin outside the exit of the
tunnel to the muscles is left open to allow drainage and discharge (3-4 weeks
duration) which then heals slowly. |
|


{kind=link}